
This series of posts is a record
of the steps that I am taking to fix my broken heart.
Before proceeding, a reminder that, in Canada February is Heart Month.
The Heart and Stroke Foundation focuses on canvassing to raise funds for research and support of people who are dealing with heart disease and strokes
 |
| Heart And Stroke Foundation |
The Heart and Stroke Foundation focuses on canvassing to raise funds for research and support of people who are dealing with heart disease and strokes
The first post in the series covered Step
1:
Find
out it's broken (diagnosis).
This post describes Step 2:Talk
to a cardiac surgeon
It's a serious problem: I finished the "Step 1" post with the confirmed diagnosis via an echocardiogram on January 22nd. I had been told that I would have to wait until a doctor's visit scheduled for February 5 before I got the results of the "echo".
When the technician was finished the test I said "So I guess I have to wait for the doctor's appointment to get the results?" He said "Yes" and then asked "When is that?". I replied two weeks. He said "Finish putting your shirt on and then come out" and he left the room.
In less than a minute he was back with the doctor who said "The results show the valve needs to be replaced - I will refer you to a cardiac surgeon in Sudbury" -- he said the narrowing (stenosis) was severe.
Waiting again but not as long as we thought: I "guessed" that the technician was able to tell that it was serious and had decided to inform the doctor so more time would be lost in waiting and -- what ever the reason -- I was thanking God that it was moving ahead -- because it's really tough waiting for answers once the test has been completed.
I was told that I would hear from the surgeon in 2 to 3 weeks so I was (again) pleasantly surprised when I got a call from the surgeon's office on Friday for the "consult" on Thursday January 31.
 "Snow" way to travel: Three and a half hours on snow covered roads isn't my idea of fun but it wasn't as bad as had been forecast - so we made the trip pretty much as "normal" speeds (i.e speed limit or slightly below -- not my summertime speeds which I'll confess are often 10- 15% above the posted limit (90 km/hour or 55 mph outside the towns -- never go over in the reduced limits unless you want the OPP flagging you down!!) (We didn't take a picture - The forecast was for "snow packed" roads with snow flurries - there wasn't any snow falling flurries or otherwise. Anyone from Northern Ontario will understand what I mean when I say we had mostly "track bare with a few snow-packed sections" but for those from more friendly climates this picture (taken from theWeathernetwork photo gallery) shows what we were dealing with. (It's NOT Northern Ontario and I forgot to note location before I saved it. When I went back I couldn't find it again.Sigh ...)
"Snow" way to travel: Three and a half hours on snow covered roads isn't my idea of fun but it wasn't as bad as had been forecast - so we made the trip pretty much as "normal" speeds (i.e speed limit or slightly below -- not my summertime speeds which I'll confess are often 10- 15% above the posted limit (90 km/hour or 55 mph outside the towns -- never go over in the reduced limits unless you want the OPP flagging you down!!) (We didn't take a picture - The forecast was for "snow packed" roads with snow flurries - there wasn't any snow falling flurries or otherwise. Anyone from Northern Ontario will understand what I mean when I say we had mostly "track bare with a few snow-packed sections" but for those from more friendly climates this picture (taken from theWeathernetwork photo gallery) shows what we were dealing with. (It's NOT Northern Ontario and I forgot to note location before I saved it. When I went back I couldn't find it again.Sigh ...)
What the surgeon said: He started with "The stenosis is severe and the surgery needs to be done as soon as possible". He proceeded with his "due diligence" to explain the surgery and the associated risks and ended with "However you are healthy otherwise so it should go well -- but it is major surgery and I need you to be aware of risks and give informed consent" blah, blah, blah, the usual "doctor speak before surgery -- I've have 4 other relatively minor surgeries so I knew that drill.
Agreeing to proceed and signing the consent form was, for us, a "no brainer" -- however I did want (perhaps my analystical, engineering brain kicked in here) to know what they meant by "severe" .
Wow -now that's severe alright! He proceeded to explain that with the echocardiogram they are able to calculate the pressure gradient across the valve and the size of the valve opening. Now he was talking my language. After all, I had just finished teaching a first year course in physics that had touched on fluid dynamics.
 In a normal aortic valve it opens fully and there is almost no pressure drop through the valve. If there is a 40% drop the valve should be replaced. Mine averaged 59% with bursts much higher.
In a normal aortic valve it opens fully and there is almost no pressure drop through the valve. If there is a 40% drop the valve should be replaced. Mine averaged 59% with bursts much higher.
The fully open normal valve has a cross sectional area of around 2.5 cm squared. They replace when it gets below 1 -- mine is 0.39 !
Now I understood what they meant by severe. There were some other results of the echo showing thickening (hyertrophy) of the ventricle (muscle) wall, and distortion (distension) of the ventricle (chamber). These caused by the increased pressures inside the ventricle.
Also some "ballooning" (distension) of the aorta just above the valve (caused by the high velocity "jet" exiting the narrowed valve - think putting your finger over the opening at the end of a water hose!!)
None of these were cause for serious concern and the Doctor thought they would "self-correct" after the valve replacement.
What's a healthy guy like you doing in a place like this: The surgeon affirmed what the cardiologists had said: There's nothing you could have done to prevent this. It just happens to a certain percentage of the population usually between 65 and 70 (so I'm right in the window of age!!). The good news is that I'm otherwise very healthy - no clogged arteries, no high blood pressure, do diabetes, etc., etc. -- none of the "risk factors" that would increase the likelihood of complications or future problems. Fix this and you're "good to go".
To be (organic) or not to be: The big decision was the choice of valve type. There are two (major) options

It's a serious problem: I finished the "Step 1" post with the confirmed diagnosis via an echocardiogram on January 22nd. I had been told that I would have to wait until a doctor's visit scheduled for February 5 before I got the results of the "echo".
When the technician was finished the test I said "So I guess I have to wait for the doctor's appointment to get the results?" He said "Yes" and then asked "When is that?". I replied two weeks. He said "Finish putting your shirt on and then come out" and he left the room.
In less than a minute he was back with the doctor who said "The results show the valve needs to be replaced - I will refer you to a cardiac surgeon in Sudbury" -- he said the narrowing (stenosis) was severe.
Waiting again but not as long as we thought: I "guessed" that the technician was able to tell that it was serious and had decided to inform the doctor so more time would be lost in waiting and -- what ever the reason -- I was thanking God that it was moving ahead -- because it's really tough waiting for answers once the test has been completed.
I was told that I would hear from the surgeon in 2 to 3 weeks so I was (again) pleasantly surprised when I got a call from the surgeon's office on Friday for the "consult" on Thursday January 31.

What the surgeon said: He started with "The stenosis is severe and the surgery needs to be done as soon as possible". He proceeded with his "due diligence" to explain the surgery and the associated risks and ended with "However you are healthy otherwise so it should go well -- but it is major surgery and I need you to be aware of risks and give informed consent" blah, blah, blah, the usual "doctor speak before surgery -- I've have 4 other relatively minor surgeries so I knew that drill.
Agreeing to proceed and signing the consent form was, for us, a "no brainer" -- however I did want (perhaps my analystical, engineering brain kicked in here) to know what they meant by "severe" .
Wow -now that's severe alright! He proceeded to explain that with the echocardiogram they are able to calculate the pressure gradient across the valve and the size of the valve opening. Now he was talking my language. After all, I had just finished teaching a first year course in physics that had touched on fluid dynamics.
 In a normal aortic valve it opens fully and there is almost no pressure drop through the valve. If there is a 40% drop the valve should be replaced. Mine averaged 59% with bursts much higher.
In a normal aortic valve it opens fully and there is almost no pressure drop through the valve. If there is a 40% drop the valve should be replaced. Mine averaged 59% with bursts much higher. The fully open normal valve has a cross sectional area of around 2.5 cm squared. They replace when it gets below 1 -- mine is 0.39 !
Now I understood what they meant by severe. There were some other results of the echo showing thickening (hyertrophy) of the ventricle (muscle) wall, and distortion (distension) of the ventricle (chamber). These caused by the increased pressures inside the ventricle.
Also some "ballooning" (distension) of the aorta just above the valve (caused by the high velocity "jet" exiting the narrowed valve - think putting your finger over the opening at the end of a water hose!!)
None of these were cause for serious concern and the Doctor thought they would "self-correct" after the valve replacement.
What's a healthy guy like you doing in a place like this: The surgeon affirmed what the cardiologists had said: There's nothing you could have done to prevent this. It just happens to a certain percentage of the population usually between 65 and 70 (so I'm right in the window of age!!). The good news is that I'm otherwise very healthy - no clogged arteries, no high blood pressure, do diabetes, etc., etc. -- none of the "risk factors" that would increase the likelihood of complications or future problems. Fix this and you're "good to go".
To be (organic) or not to be: The big decision was the choice of valve type. There are two (major) options
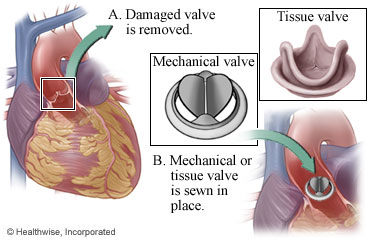
- a mechanical valve which lasts a lifetime but requires a lifetime regime of taking a blood thinner to prevent clots (and has a higher risk of bleeding and/or stroke )
- a tissue valve (in this case a valve constructed from bovine pericardial tissue, (the tough tissue sac that surrounds the heart of a cow) which lasts for 10 to 15 years without any requirement for blood thinners (and has a higher risk of future heart disease -- and possible need for another surgery --- when the valve begins to fail).
The Doctor says less if you are younger than 55 or need to take blood thinners anyhow for other reasons you should chooses a mechanical valve for sure and if you are older than 70 then you should choose a tissue valve for sure. I'm in between and (as my lovely wife is kind enough to say) a young 68.
However, I more inclined to go with immediate benefit of no ongoing medication and increased risk of stroke rather than the POSSIBILITY of future problems so out choice is to use the tissue valve.
(I did have some second thoughts after we got home and did a fair amount of research which at the end confirmed my comfort with the choice. I was particularly influenced by 2 factors
- I found some recent studies that suggest that for people over 65 over 95% of tissue valves are fine after 20 years
- There are emerging "minimally invasive" techniques for valve replacement and even one that uses same process as is used for inserting artery stents that is done via inserting a catheter through the groin. So who's to say if the valve starts failing in 10 years that these methods won'y be more "routinely" available.
Go home and wait some more: Having agreed to the surgery, discussed the severity of the stentosis and its side effects AND picked the valve - we asked "When?".
It seemed to us the sooner the better. The doctor sais he would inform the cardiac surgery coordinator at the hospital and they would get back to us. He said it was difficult to say how long because there could be emergency or other higher priority surgergies that came up but he expected the surgery would occur in 3 to 6 weeks.
That was a bit challenging for us -- especially Linda since , with her medical knowledge, she was concerned of the risk of sudden cardiac arrest in the meantime and one of the less-than-comforting facts the surgeon had explained to us was that if I had cardiac arrest for any reason it would be highly unlikely that the heart could be re-started (for the mechanical minded think about trying to re-start a water pump if the outlet valve is clogged!)
The trip home was uneventful (other than the challenges of the last 2 hours being after dark and some issues with getting the windshield properly cleaned and cleaning the grit of the headlights so she could see the road -- that was a kind of Gen. 1:3 moment for her :)
Certainly we were both anxious to get the surgery scheduled
Continued to-morrow
God Bless
Charlie

No comments:
Post a Comment